
Proficiency and Interlaboratory Variability in the Determination of Phthalate and DINCH Biomarkers in Human Urine: Results from the HBM4EU Project

 , ,
, ,  ,
,  , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of the HBM4EU QA/QC Program
2.2. Preparation and Characterization of Control Materials
2.3. Organization of Proficiency Tests
2.4. Assessment of Laboratory Performance
2.4.1. Quantitative Performance
2.4.2. False Negatives and False Positives
3. Results and Discussion
3.1. Homogeneity and Stability Testing
3.2. Values for the Expert Laboratories
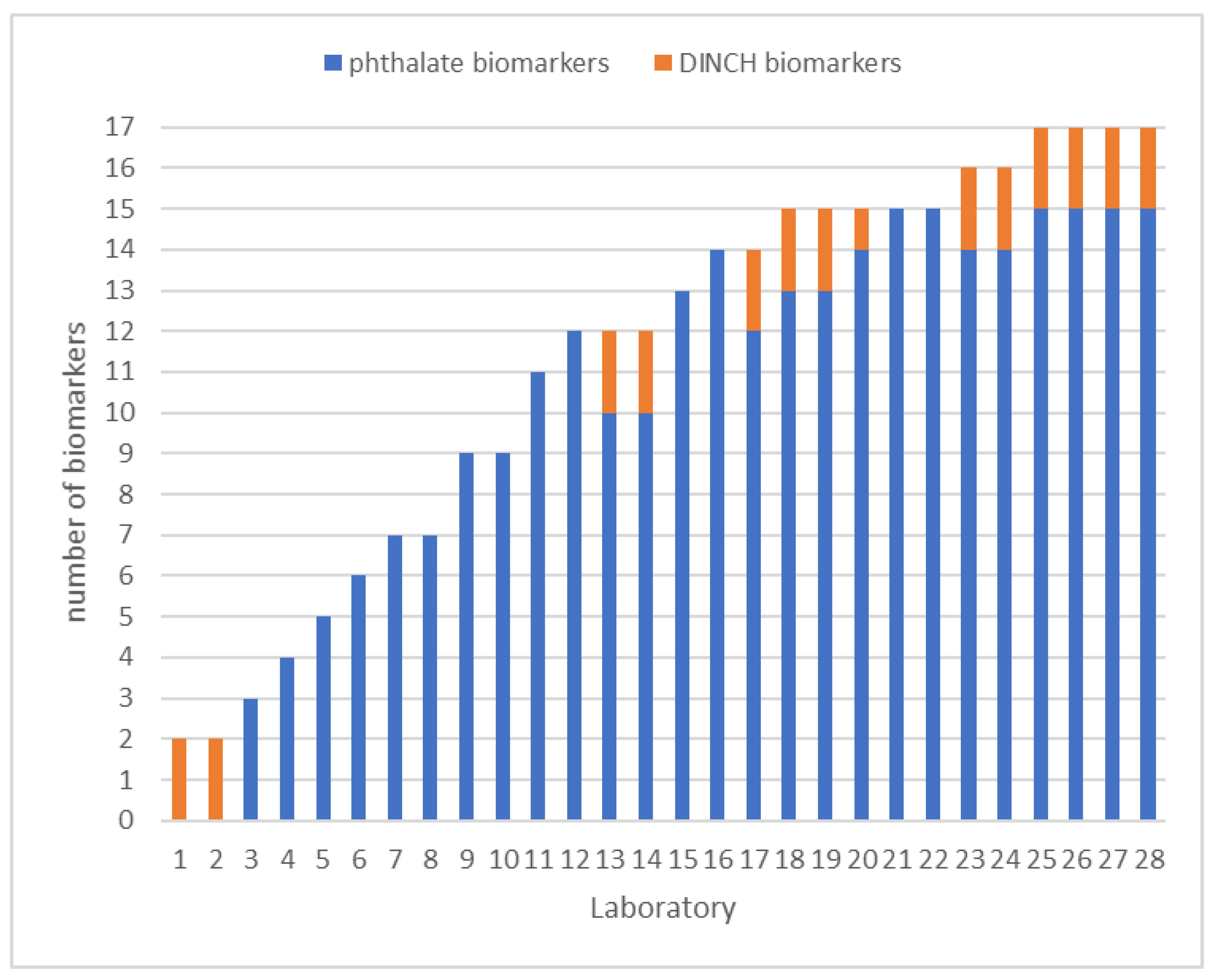
3.3. Participants’ Scope, LOQs, and Methods
3.4. Assessment of Laboratory Performance
3.4.1. First Round Experiences
- Background contamination. In the cases of the monoesters (MEP, MBzP, MnBP, MiBP, and MEHP), external contamination may occur which may cause a positively biased result, especially at the lower concentrations. Careful monitoring by inclusion of multiple procedural blanks can reveal this. If it occurs, the source should be identified and measures taken to prevent background artefacts.
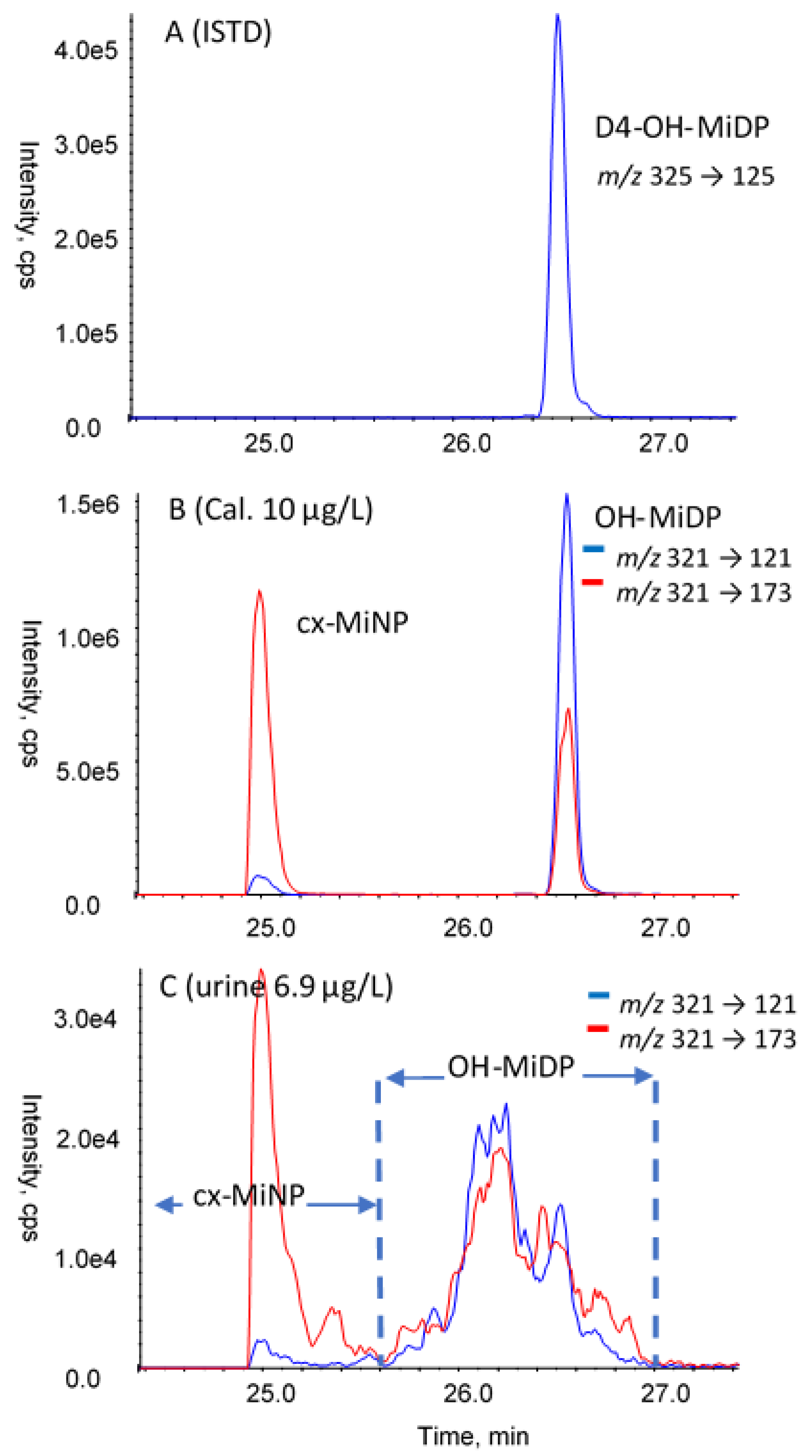
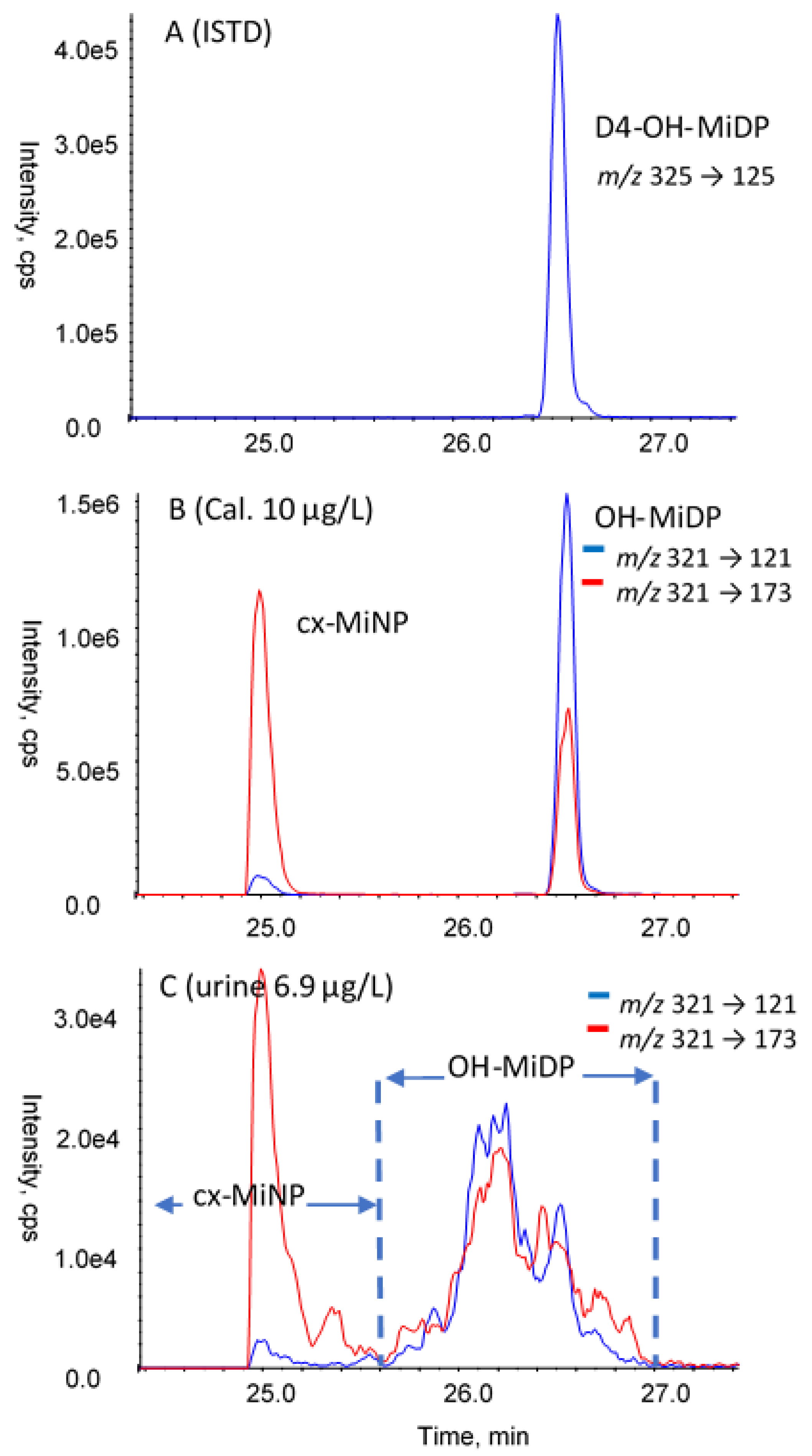
- Peak separation and integration. For MnBP/MiBP, the LC-MS/MS separation is dif-ficult and integration needs attention. For DiNP, DiDP, and DINCH, the biomarkers in real samples originate from isomeric parent compound mixtures. While the analytical (internal) standards yield one defined chromatographic peak, multiple and/or broad peaks are observed in real samples. During the measurement, the acquisition window for these compounds needs to be sufficiently wide to capture the complete mixture. Care needs to be taken during data processing to include all peaks (for example, see Figure 4). Another issue is that for the isomer mixtures, the transition used for quantification affects the quantitative result. For this reason, in the subsequent rounds, the laboratories were instructed to use harmonized quantifier m/z transitions (OH-MiNP: 307 > 121; cx MiNP: 321 > 173; OH-MiDP: 321 > 121; cx-MiDP: 335 > 187; OH-MINCH: 313 > 153; cx-MINCH: 327 > 173).
- Internal standard used. All laboratories used internal standards to correct for possible losses or inconsistencies during sample preparation, and to correct for matrix effects in the LC-MS/MS measurement. Especially for the latter, the best option is to use the isotope-labelled analogue for each of the biomarkers analyzed, because matrix effects can be highly variable for the different analytes and the different urine samples. In a substantial number of cases, other isotope-labelled internal standards were used, or even a single isotope-labelled internal standard for all biomarkers analyzed. This may result in sub-optimal or even erroneous correction for matrix effects and deviating analysis results. To illustrate this, the performance obtained with or without using the corresponding isotope-labelled analogue were compared (only results with full details on internal standards used were included). A summary is provided in Table 4. Although satisfactory performance could still be obtained using other internal standards, in all four rounds the results relating to the use of the authentic isotope-labelled analogue were better.
- Enzyme used for deconjugation. Phthalate and DINCH biomarkers in urine of exposed subjects are predominantly present as glucuronides, depending on alkyl chain length and type of oxidative modification [38,39]. HBM analysis is based on the determination of the total aglycone concentration after cleavage of the conjugates. In the cases of phthalates and their substitutes, deconjugation needs to be done carefully because of their labile ester bond(s), which is usually achieved by enzymatic hydrolyses. The type of enzyme, its concentration, pH, and time may affect the resulting concentration of the aglycone. It has been recommended to use pure β-glucuronidase (e.g., from E. coli K12) rather than lesser defined or mixed enzyme types such as Helix Pomatia β-glucuronidase/aryl sulfatase. While both will result in deglucuronidation, sulfatase/lipase activities present in mixed enzymes from H. Pomatia may both cleave the ester-bonds of phthalates (and DINCH) and their biomarkers [40,41]. Thus, early on, phthalate HBM methods were successfully based on ß-glucuronidase-pure enzymes [18,19,40]. However, as indicated in Table 2, roughly a quarter (28%) of the laboratories used enzymes from H. Pomatia for deconjugation. It was investigated whether a difference in results could be observed between the laboratories using E. coli- and H. Pomatia- based enzymes. For this purpose, the data from round-2 were used (highest number of participants). To eliminate bias due to matrix effects in the LC-MS/MS measurement, results were only included when the corresponding isotope-labelled analogue was used as the internal standard in the determination. An additional requirement was that at least three results were available for both groups. A comparison could be made for seven biomarkers in two control materials. The results are included in the supplementary material (Table S5 and Figure S1). For the low-concentration control material R2A, the use of enzymes from H. Pomatia resulted in significantly higher concentrations of the simple monoester biomarkers MiBP, MnBP, and MEHP (35%, 49%, and 120%, respectively). This could be explained by the parent diester (that is ubiquitously present) being degraded to the simple monoester, thus artificially elevating their concentrations in the low-concentration control samples. In the high concentration samples, this contribution might be less relevant. In fact, for material R2B, the concentrations reported with H. Pomatia appeared slightly lower (less than 20% and therefore not significant), which could be the result of analyte loss through esterase activity in enzyme preparations from H. Pomatia. Thus, it seems that the use of H. Pomatia results in a positive bias of some biomarkers in the low concentration materials (R2A), and similar results or a negative bias in the high concentration control materials. To summarize, the use of β-glucuronidase pure enzymes is strongly recommended for the determination of phthalate and DINCH biomarkers because: (i) degradation issues related to the arylsulfatase component of mixed enzymes are obvious (resulting in a myriad of quantitatively interfering effects, especially obvious for the monoesters MnBP, MiBP, and MEHP), (ii) human phthalate metabolism data and urinary excretion fractions are based on methods using arylsulfatase-free glucuronidase enzymes, and (iii) most laboratories (including expert laboratories) use these enzymes.
3.4.2. Laboratory Performances along the HBM4EU QA/QC Program
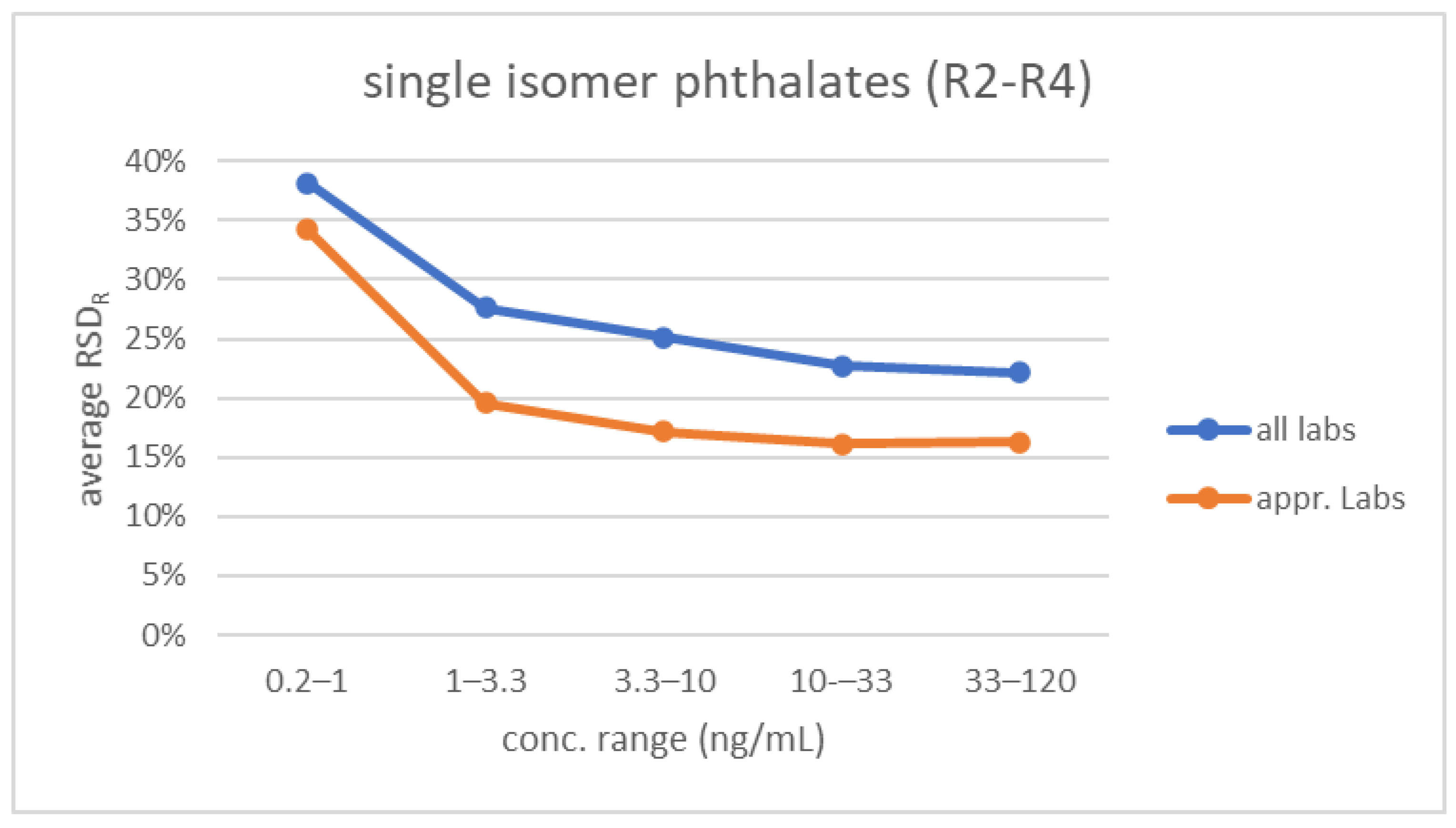
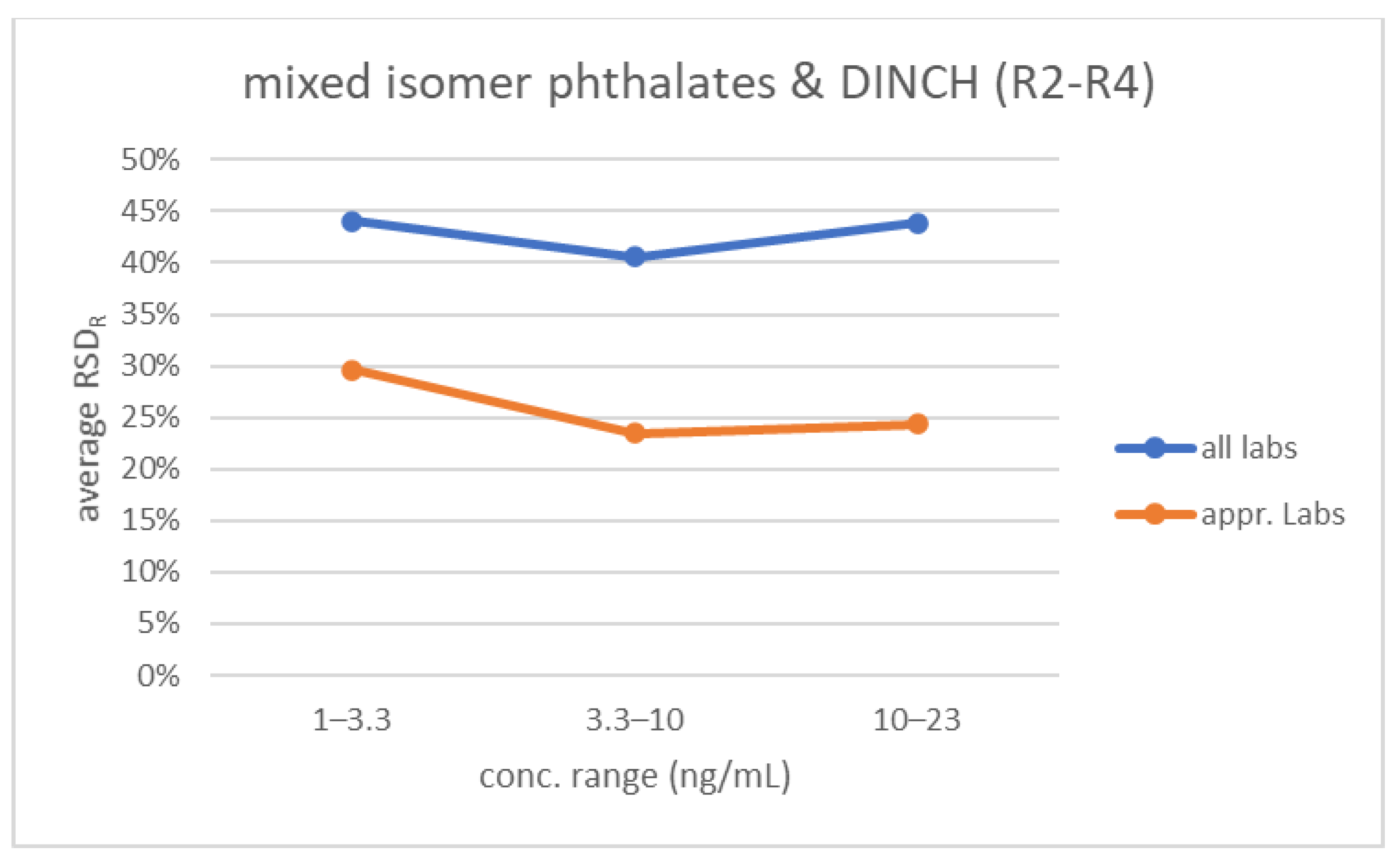
3.5. Interlaboratory Variability
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Fisher, J.S. Environmental anti-androgens and male reproductive health: Focus on phthalates and testicular dysgenesis syndrome. Reproduction 2004, 127, 305–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furr, J.R.; Lambright, C.S.; Wilson, V.S.; Foster, P.M.; Gray, L.E., Jr. A Short-term In Vivo Screen Using Fetal Testosterone Production, a Key Event in the Phthalate Adverse Outcome Pathway, to Predict Disruption of Sexual Differentiation. Toxicol. Sci. 2014, 140, 403–424. [Google Scholar] [CrossRef] [PubMed]
- Lioy, P.J.; Hauser, R.; Gennings, C.; Koch, H.M.; Mirkes, P.E.; Schwetz, B.A.; Kortenkamp, A. Assessment of phthalates/phthalate alternatives in children’s toys and childcare articles: Review of the report including conclusions and recommendation of the Chronic Hazard Advisory Panel of the Consumer Product Safety Commission. J. Exp. Sci. Environ. Epidemiol. 2015, 25, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Howdeshell, K.L.; Hotchkiss, A.K.; Earl Gray, L., Jr. Cumulative effects of antiandrogenic chemical mixtures and their relevance to human health risk assessment. Int. J. Hyg. Environ. Health 2017, 220, 179–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kortenkamp, A.; Koch, H.M. Refined reference doses and new procedures for phthalate mixture risk assessment focused on male developmental toxicity. Int. J. Hyg. Environ. Health 2020, 224, 113428. [Google Scholar] [CrossRef]
- Koch, H.M.; Rüther, M.; Schütze, A.; Conrad, A.; Pälmke, C.; Apel, P.; Brüning, T.; Kolossa-Gehring, M. Phthalate metabolites in 24-h urine samples of the German Environmental Specimen Bank (ESB) from 1988 to 2015 and a comparison with US NHANES data from 1999 to 2012. Int. J. Hyg. Environ. Health 2017, 220, 130–141. [Google Scholar] [CrossRef] [Green Version]
- Zota, A.R.; Calafat, A.M.; Woodruff, T.J. Temporal trends in phthalate exposures: Findings from the National Health and Nutrition Examination Survey, 2001–2010. Environ. Health Perspect. 2014, 122, 235–241. [Google Scholar] [CrossRef] [Green Version]
- Kasper-Sonnenberg, M.; Koch, H.M.; Apel, P.; Rüther, M.; Pälmke, C.; Brüning, T.; Kolossa-Gehring, M. Time trend of exposure to the phthalate plasticizer substitute DINCH in Germany from 1999 to 2017: Biomonitoring data on young adults from the Environmental Specimen Bank (ESB). Int. J. Hyg. Environ. Health 2019, 222, 1084–1092. [Google Scholar] [CrossRef]
- Lessmann, F.; Kolossa-Gehring, M.; Apel, P.; Rüther, M.; Pälmke, C.; Harth, V.; Brüning, T.; Koch, H. German Environmental Specimen Bank: 24-hour urine samples from 1999 to 2017 reveal rapid increase in exposure to the para-phthalate plasticizer di(2-ethylhexyl) terephthalate (DEHTP). Environ. Int. 2019, 132, 105102. [Google Scholar] [CrossRef]
- Schmidtkunz, C.; Gries, W.; Weber, T.; Leng, G.; Kolossa-Gehring, M. Internal exposure of young German adults to di(2-propylheptyl) phthalate (DPHP): Trends in 24-h urine samples from the German Environmental Specimen Bank 1999–2017. Int. J. Hyg. Environ. Health 2019, 222, 419–424. [Google Scholar] [CrossRef]
- Frederiksen, H.; Nielsen, O.; Koch, H.M.; Skakkebaek, N.E.; Juul, A.; Jørgensen, N.; Andersson, A.M. Changes in urinary excretion of phthalates, phthalate substitutes, bisphenols and other polychlorinated and phenolic substances in young Danish men; 2009–2017. Int. J. Hyg. Environ. Health 2020, 223, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Bastiaensen, M.; Gys, C.; Colles, A.; Malarvannan, G.; Verheyen, V.; Koppen, G.; Govarts, E.; Bruckers, L.; Morrens, B.; Franken, C.; et al. Biomarkers of phthalates and alternative plasticizers in the Flemish Environment and Health Study (FLEHS IV): Time trends and exposure assessment. Environ. Pollut. 2021, 276, 116724. [Google Scholar] [CrossRef] [PubMed]
- Apel, P.; Kortenkamp, A.; Koch, H.M.; Vogel, N.; Rüther, M.; Kasper-Sonnenberg, M.; Conrad, A.; Brüning, T.; Kolossa-Gehring, M. Time course of phthalate cumulative risks to male developmental health over a 27-year period: Biomonitoring samples of the German Environmental Specimen Bank. Environ. Int. 2020, 137, 105467. [Google Scholar] [CrossRef] [PubMed]
- Fréry, N.; Santonen, T.; Porras, S.P.; Fucic, A.; Leso, V.; Bousoumah, R.; Duca, R.C.; El Yamani, M.; Kolossa-Gehring, M.; Ndaw, S.; et al. Biomonitoring of occupational exposure to phthalates: A systematic review. Int. J. Hyg. Environ. Health 2020, 229, 113548. [Google Scholar] [CrossRef] [PubMed]
- Schwedler, G.; Rucic, E.; Lange, R.; Conrad, A.; Koch, H.M.; Pälmke, C.; Brüning, T.; Schulz, C.; Schmied-Tobies, M.I.H.; Daniels, A.; et al. Phthalate metabolites in urine of children and adolescents in Germany. Human biomonitoring results of the German Environmental Survey GerES V, 2014–2017. Int. J. Hyg. Environ. Health 2020, 225, 113444. [Google Scholar] [CrossRef] [PubMed]
- Lange, R.; Apel, P.; Rousselle, C.; Charles, S.; Sissoko, F.; Kolossa-Gehring, M.; Ougier, E. The European Human Biomonitoring Initiative (HBM4EU): Human biomonitoring guidance values for selected phthalates and a substitute plasticizer. Int. J. Hyg. Environ. Health 2021, 234, 113722. [Google Scholar] [CrossRef]
- Lemke, N.; Murawski, A.; Lange, R.; Weber, T.; Apel, P.; Dębiak, M.; Koch, H.M.; Kolossa-Gehring, M. Substitutes mimic the exposure behaviour of REACH regulated phthalates—A review of the German HBM system on the example of plasticizers. Int. J. Hyg. Environ. Health 2021, 236, 113780. [Google Scholar] [CrossRef]
- Barr, D.B.; Silva, M.J.; Kato, K.; Reidy, J.A.; Malek, N.A.; Hurtz, D.; Sadowski, M.; Needham, L.L.; Calafat, A.M. Assessing human exposure to phthalates using monoesters and their oxidized metabolites as biomarkers. Environ. Health Perspect. 2003, 111, 1148–1151. [Google Scholar] [CrossRef]
- Koch, H.M.; Gonzalez-Reche, L.M.; Angerer, J. On-line clean-up by multidimensional liquid chromatography-electrospray ionization tandem mass spectrometry for high throughput quantification of primary and secondary phthalate metabolites in human urine. J. Chromatogr. B Analyt. Technol. Biomed Life Sci. 2003, 784, 169–182. [Google Scholar] [CrossRef]
- Silva, M.J.; Samandar, E.; Preau JLJr Reidy, J.A.; Needham, L.L.; Calafat, A.M. Quantification of 22 phthalate metabolites in human urine. J. Chromatogr. B Analyt. Technol. Biomed Life Sci. 2007, 860, 106–112. [Google Scholar] [CrossRef]
- Schütze, A.; Pälmke, C.; Angerer, J.; Weiss, T.; Brüning, T.; Koch, H.M. Quantification of biomarkers of environmental exposure to di(isononyl)cyclohexane-1,2-dicarboxylate (DINCH) in urine via HPLC-MS/MS. J. Chromatogr. B Analyt. Technol. Biomed Life Sci. 2012, 895–896, 123–130. [Google Scholar] [CrossRef]
- Wittassek, M.; Angerer, J.; Kolossa-Gehring, M.; Schäfer, S.D.; Klockenbusch, W.; Dobler, L.; Günsel, A.K.; Müller, A.; Wiesmüller, G.A. Fetal exposure to phthalates—A pilot study. Int. J. Hyg. Environ. Health 2009, 212, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Koch, H.M.; Calafat, A.M. Human body burdens of chemicals used in plastic manufacture. Philos. Trans. R. Soc. B Biol. Sci. 2009, 364, 2063–2078. [Google Scholar] [CrossRef] [PubMed]
- Calafat, A.M.; Longnecker, M.P.; Koch, H.M.; Swan, S.H.; Hauser, R.; Goldman, L.R.; Lanphear, B.P.; Rudel, R.A.; Engel, S.M.; Teitelbaum, S.L.; et al. Optimal Exposure Biomarkers for Nonpersistent Chemicals in Environmental Epidemiology. Environ. Health Perspect. 2015, 123, A166–A168. [Google Scholar] [CrossRef] [PubMed]
- Vorkamp, K.; Castaño, A.; Antignac, J.-P.; Boada, L.D.; Cequier, E.; Covaci, A.; Esteban López, M.; Haug, L.S.; Kasper-Sonnenberg, M.; Koch, H.M.; et al. Biomarkers, matrices and analytical methods targeting human exposure to chemicals selected for a European human biomonitoring initiative. Environ. Int. 2021, 146, 106082. [Google Scholar] [CrossRef]
- Schindler, B.K.; Esteban, M.; Koch, H.M.; Castano, A.; Koslitz, S.; Canas, A.; Casteleyn, L.; Kolossa-Gehring, M.; Schwedler, G.; Schoeters, G.; et al. The European COPHES/DEMOCOPHES project: Towards transnational comparability and reliability of human biomonitoring results. Int. J. Hyg. Environ. Health 2014, 217, 653–661. [Google Scholar] [CrossRef]
- Den Hond, E.; Govarts, E.; Willems, H.; Smolders, R.; Casteleyn, L.; Kolossa-Gehring, M.; Schwedler, G.; Seiwert, M.; Fiddicke, U.; Castaño, A.; et al. First steps toward harmonized human biomonitoring in Europe: Demonstration project to perform human biomonitoring on a European scale. Environ. Health Perspect. 2015, 123, 255–263. [Google Scholar] [CrossRef] [Green Version]
- Schantz, M.M.; Benner, B.A., Jr.; Heckert, N.A.; Sander, L.C.; Sharpless, K.E.; Vander Pol, S.S.; Vasquez, Y.; Villegas, M.; Wise, S.A.; Alwis, K.U.; et al. Development of urine standard reference materials for metabolites of organic chemicals including polycyclic aromatic hydrocarbons, phthalates, phenols, parabens, and volatile organic compounds. Anal. Bioanal. Chem. 2015, 407, 2945–2954. [Google Scholar] [CrossRef]
- Ganzleben, C.; Antignac, J.P.; Barouki, R.; Castaño, A.; Fiddicke, U.; Klánová, J.; Lebret, E.; Olea, N.; Sarigiannis, D.; Schoeters, G.R.; et al. Human biomonitoring as a tool to support chemicals regulation in the European Union. Int. J. Hyg. Environ. Health 2017, 220, 94–97. [Google Scholar] [CrossRef]
- Esteban López, M.; Göen, T.; Mol, H.; Nübler, S.; Zarrabi, K.; Koch, H.M.; Dvorakova, D.; Hajslova, J.; Antignac, J.P.; Vacher, V.; et al. The European Human Biomonitoring platform—Design and implementation of a QA/QC programme for selected priority chemicals. Int. J. Hyg. Environ. Health 2021, 234, 113740. [Google Scholar] [CrossRef]
- Machtinger, R.; Gaskins, A.J.; Racowsky, C.; Mansur, A.; Adir, M.; Baccarelli, A.A.; Calafat, A.M.; Hauser, R. Urinary concentrations of biomarkers of phthalates and phthalate alternatives and IVF outcomes. Environ. Int. 2018, 111, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Schwedler, G.; Conrad, A.; Rucic, E.; Koch, H.M.; Leng, G.; Schulz, C.; Schmied-Tobies, M.I.H.; Kolossa-Gehring, M. Hexamoll® DINCH and DPHP metabolites in urine of children and adolescents in Germany. Human biomonitoring results of the German Environmental Survey GerES V, 2014–2017. Int. J. Hyg. Environ. Health 2020, 229, 113397. [Google Scholar] [CrossRef] [PubMed]
- ISO 13528:2015; Statistical Methods for Use in Proficiency Testing by Interlaboratory Comparison. ISO: Geneva, Switzerland, 2015.
- Fearn, T.; Thompson, M. A new test for ‘sufficient homogeneity’. Analyst 2001, 126, 1414–1417. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.; Ellison, R.; Wood, R. The International Harmonized Protocol for the Proficiency Testing of Analytical Chemistry Laboratories. Pure Appl. Chem. 2006, 78, 145–196. [Google Scholar] [CrossRef]
- Philippat, C.; Rolland, M.; Lyon-Caen, S.; Pin, I.; Sakhi, A.K.; Sabaredzovic, A.; Thomsen, C.; Slama, R. Pre- and early post-natal exposure to phthalates and DINCH in a new type of mother-child cohort relying on within-subject pools of repeated urine samples. Environ. Pollut. 2021, 287, 117650. [Google Scholar] [CrossRef]
- Runkel, A.A.; Mazej, D.; Snoj Tratnik, J.; Tkalec, Ž.; Kosjek, T.; Horvat, M. Exposure of men and lactating women to environmental phenols, phthalates, and DINCH. Chemosphere 2021, 286, 131858. [Google Scholar] [CrossRef]
- Samandar, E.; Silva, M.J.; Reidy, J.A.; Needham, L.L.; Calafat, A.M. Temporal stability of eight phthalate metabolites and their glucuronide conjugates in human urine. Environ. Res. 2009, 109, 641–646. [Google Scholar] [CrossRef]
- Koch, H.M.; Schütze, A.; Pälmke, C.; Angerer, J.; Brüning, T. Metabolism of the plasticizer and phthalate substitute diisononyl-cyclohexane-1,2-dicarboxylate (DINCH®) in humans after single oral doses. Arch. Toxicol. 2013, 87, 799–806. [Google Scholar] [CrossRef]
- Blount, B.C.; Silva, M.J.; Caudill, S.P.; Needham, L.L.; Pirkle, J.L.; Sampson, E.J.; Lucier, G.W.; Jackson, R.J.; Brock, J.W. Levels of seven urinary phthalate metabolites in a human reference population. Environ. Health Perspect. 2000, 108, 979–982. [Google Scholar] [CrossRef]
- Koch, H.M.; Lessmann, F.; Swan, S.H.; Hauser, R.; Kolossa-Gehring, M.; Frederiksen, H.; Andersson, A.-M.; Thomsen, C.; Sakhi, A.K.; Bornehag, G.C.-G.; et al. Analyzing terephthalate metabolites in human urine as biomarkers of exposure: Importance of selection of metabolites and deconjugation enzyme. J. Chromatogr. B 2018, 1100–1101, 91–92. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parent Compound | Biomarker(s) | Abbreviation |
|---|---|---|
| Phthalates | ||
| Diethyl phthalate (DEP) | Mono-ethyl phthalate | MEP |
| Butyl benzyl phthalate (BBzP) | Mono-benzyl phthalate | MBzP |
| Di-isobutyl phthalate (DiBP) | Mono-isobutyl phthalate | MiBP |
| Di-n-butyl phthalate (DnBP) | Mono-n-butyl phthalate | MnBP |
| Dicyclo-hexyl phthalate (DCHP) | Mono-cyclo-hexyl phthalate | MCHP |
| Di-n-pentyl phthalate (DnPeP) | Mono-n-pentyl phthalate | MnPeP |
| Di(2-ethylhexyl)phthalate (DEHP) | Mono(2-ethylhexyl) phthalate | MEHP |
| Mono(2-ethyl-5-hydroxy-hexyl) phthalate | 5OH-MEHP | |
| Mono(2-ethyl-5-oxo-hexyl) phthalate | 5oxo-MEHP | |
| Mono(2-ethyl-5-carboxy-pentyl) phthalate | 5cx-MEPP | |
| Di-n-octyl phthalate (DnOP) | Mono-n-octyl phthalate | MnOP |
| Di-isononyl phthalate (DiNP) | 7-OH-(mono-methyl-octyl) phthalate | OH-MiNP |
| 7-Carboxy-(mono-methyl-heptyl) phthalate | cx-MiNP | |
| Di-isodecyl phthalate (DiDP) 1 | 6-OH-Mono-propyl-heptyl phthalate | OH-MiDP |
| Mono(2,7-methyl-7-carboxy-heptyl) phthalate | cx-MiDP | |
| Alternatives: DINCH | ||
| Di-isononyl cyclohexane-1,2-dicarboxylate (DINCH) | cyclohexane-1,2-dicarboxylate-mono-(7-hydroxy-4-methyl)octyl ester | OH-MINCH |
| cyclohexane-1,2-dicarboxylate-mono-(7-carboxylate-4-methyl)heptyl ester | cx-MINCH |
| Step | Details and Usage by the Laboratories |
|---|---|
| Pretreatment of urine | none (92%) centrifugation (8%) |
| Urine aliquot used | 0.1–3.0 mL, median 0.5 mL |
| pH adjustment before deconj. | buffer added, in most cases Na/NH4 acetate buffer, pH 6.5 |
| Deconjugation | enzymatic in all cases: E. coli-based β-glucuronidase, 37 °C, 0.5–15 h, median 2 h (72%) Helix Pomatia-based (β-glucuronidase/sulfatase), 37 °C, 1–2 h or overnight (28%) |
| Sample adjustment before extraction | acidification with formic acid or acetic acid (67%) none (33%) |
| Extraction/cleanup | SPE online (40%), SPE off-line (28%), LLE (8%) none/dilute and shoot (24%) |
| Instrumental analysis | LC-MS/MS (ESI negative mode) (96%) GC-MS after derivatization (4%) |
| Internal standards used | corresponding isotope-labelled analogue for each biomarker (54%) isotope-labelled biomarker, partially corresponding/partially not (27%) isotope labels used not specified at individual biomarker level (12%) no information provided (8%) |
| Moment of addition of internal standard to sample | before deconjugation (96%) before extraction (4%) |
| Quantification | response normalized to internal standard (100%) calibration standards prepared in solvent/eluent (68%) procedural calibration using synthetic urine/blank urine/water (28%) standard prepared in final extract (4%) |
| Identification | |
| Retention time tolerance used | absolute: <±0.1 min (36%), ±0.1 min (28%), ±0.2–0.5 min (12%) relative, ±0.1−2.5% of ret. time (24%) not specified (8%) |
| Number of transitions acquired | 1 (24%), 2 (68%), 3 (8%) |
| Ion ratio tolerance used | ±15% (13%), ±20% (56%), ±30% (31%) |
| Biomarker | R | CM | C(E) ng/mL | C(C) ng/mL | RSDR | Δ C(C) Vs. C(E) | N (q) (<LOQ) | S | Q | US |
|---|---|---|---|---|---|---|---|---|---|---|
| MEP | 1 | A | 1 | 127 | 28% | - | 14 | 86% | 7% | 7% |
| B | 1 | 123 | 42% | - | 14 | 79% | 7% | 14% | ||
| 2 | A | 17.4 | 19.7 | 27% | 13% | 21 | 86% | 5% | 10% | |
| B | 52.3 | 59.7 | 21% | 14% | 21 | 81% | 10% | 10% | ||
| 3 | A | 71.8 | 77.5 | 17% | 8% | 20 | 85% | 5% | 10% | |
| B | 103 | 108 | 17% | 4% | 20 | 95% | 0% | 5% | ||
| 4 | A | 51.5 | 56.2 | 18% | 9% | 15 | 93% | 0% | 7% | |
| B | 122 | 128 | 22% | 5% | 15 | 93% | 0% | 7% | ||
| MBzP | 1 | A | 1 | 2.60 | 23% | - | 16 | 88% | 0% | 13% |
| B | 1 | 3.96 | 26% | - | 16 | 94% | 6% | 0% | ||
| 2 | A | 0.955 | 1.15 | 27% | 20% | 19 (2×<) | 76% | 5% | 19% | |
| B | 10.4 | 10.4 | 23% | 1% | 21 | 95% | 0% | 5% | ||
| 3 | A | <0.2 | 0.24 | 29% | - | 9 (11×<) | 4 | 4 | 4 | |
| B | 3.21 | 2.86 | 19% | −11% | 20 | 90% | 10% | 0% | ||
| 4 | A | 2.03 | 2.13 | 13% | 5% | 14 | 93% | 0% | 7% | |
| B | 2.81 | 2.98 | 8% | 6% | 14 | 93% | 0% | 7% | ||
| MiBP | 1 | A | 1 | 7.26 | 32% | - | 16 | 94% | 0% | 6% |
| B | 1 | 19.3 | 30% | - | 16 | 81% | 19% | 0% | ||
| 2 | A | 8.59 | 8.48 | 30% | −1% | 21 | 90% | 5% | 5% | |
| B | 69.9 | 65.4 | 36% | −6% | 21 | 86% | 10% | 5% | ||
| 3 | A | 1.28 | 1.45 | 39% | 13% | 16 (4×<, 2 FN) | 82% | 6% | 12% | |
| B | 15.3 | 15.1 | 19% | −1% | 20 | 95% | 0% | 5% | ||
| 4 | A | 17.4 | 17.7 | 24% | 2% | 16 | 100% | 0% | 0% | |
| B | 17.2 | 17.8 | 24% | 4% | 16 | 94% | 6% | 0% | ||
| MnBP | 1 | A | 1 | 11.1 | 26% | - | 16 | 88% | 0% | 13% |
| B | 1 | 16.4 | 31% | - | 16 | 88% | 6% | 6% | ||
| 2 | A | 6.64 | 7.63 | 29% | 15% | 21 | 86% | 5% | 10% | |
| B | 53.9 | 54.9 | 25% | 2% | 21 | 95% | 5% | 0% | ||
| 3 | A | 1.03 | 1.13 | 34% | 10% | 18 (2×<) | 89% | 6% | 6% | |
| B | 11.8 | 11.1 | 14% | −6% | 20 | 95% | 0% | 5% | ||
| 4 | A | 13.9 | 14.2 | 20% | 2% | 16 | 94% | 6% | 0% | |
| B | 11.0 | 11.3 | 25% | 3% | 16 | 94% | 6% | 0% | ||
| MCHP | 1 | A | (<0.2) 1,6 | 4 | 2 + 2 FP (7×<) | 4 | 4 | 4 | ||
| B | 1 | 0.925 | 39% | - | 10 (1×<) | 90% | 10% | 0% | ||
| 2 | A | <0.20 | 4,8 | 6 (7×<) | 4,8 | 4,8 | 4,8 | |||
| B | 1.26 | 1.43 | 33% | 13% | 13 | 92% | 8% | 0% | ||
| 3 | A | < 0.2 | 4 | 1 (12×<) | 4 | 4 | 4 | |||
| B | (0.29) 2,6 | 5 | 54% | 11 (2×<) | 7 | 7 | 7 | |||
| 4 | A | 0.295 | 0.345 | 20% | 17% | 10 (3×<) | 90% | 0% | 10% | |
| B | 0.533 | 0.625 | 24% | 17% | 10 (3×<) | 90% | 0% | 10% | ||
| MnPeP | 1 | A | (<0.2) 1,6 | 4 | 2 FP (7×<) | 4 | 4 | 4 | ||
| B | (1.43) 1,6 | 5 | 59% | - | 8 (1×<) | 7 | 7 | 7 | ||
| 2 | A | (<0.2) 2,6 | 4 | 10 (2×<) | 4 | 4 | 4 | |||
| B | (11.8) 3 | 10.4 | 49% | −12% | 12 | 75% | 25% | 0% | ||
| 3 | A | <0.2 | 4 | 0 (11×<) | 4 | 4 | 4 | |||
| B | 1.32 | 5 | 43% | - | 10 (1×<) | 80% | 10% | 10% | ||
| 4 | A | 1.75 | 2.33 | 36% | 34% | 11 (1×<) | 64% | 18% | 18% | |
| B | 2.50 | 3.06 | 19% | 22% | 12 | 83% | 0% | 17% | ||
| MEHP | 1 | A | 1 | 1.83 | 40% | - | 16 (2×<) | 75% | 6% | 19% |
| B | 1 | 8.58 | 34% | - | 18 | 83% | 11% | 6% | ||
| 2 | A | 0.567 | 1.12 | 51% | 98% | 17 (6×<) | 52% | 4% | 43% | |
| B | 5.89 | 6.75 | 28% | 15% | 23 | 87% | 4% | 9% | ||
| 3 | A | 1.21 | 1.30 | 27% | 7% | 20 | 90% | 5% | 5% | |
| B | 4.76 | 5.11 | 22% | 7% | 20 | 95% | 5% | 0% | ||
| 4 | A | 3.33 | 4.01 | 28% | 21% | 17 | 82% | 12% | 6% | |
| B | 3.98 | 4.81 | 25% | 21% | 17 | 88% | 6% | 6% | ||
| 5OH-MEHP | 1 | A | 1 | 11.3 | 26% | - | 18 | 89% | 0% | 11% |
| B | 1 | 40.1 | 24% | - | 18 | 78% | 6% | 17% | ||
| 2 | A | 4.12 | 4.12 | 21% | 0% | 23 | 100% | 0% | 0% | |
| B | 32.3 | 27.6 | 28% | −14% | 23 | 91% | 9% | 0% | ||
| 3 | A | 3.01 | 2.96 | 21% | −2% | 21 | 95% | 5% | 0% | |
| B | 27.1 | 25.4 | 14% | −6% | 21 | 100% | 0% | 0% | ||
| 4 | A | 13.2 | 13.4 | 13% | 2% | 17 | 100% | 0% | 0% | |
| B | 23.2 | 23.9 | 13% | 3% | 17 | 94% | 0% | 6% | ||
| 5oxo-MEHP | 1 | A | 1 | 5.30 | 25% | - | 18 | 89% | 6% | 6% |
| B | 1 | 18.6 | 38% | - | 18 | 83% | 17% | 0% | ||
| 2 | A | 1.74 | 1.69 | 18% | −2% | 22 (1×<) | 91% | 4% | 4% | |
| B | 14.6 | 12.5 | 18% | −14% | 23 | 87% | 13% | 0% | ||
| 3 | A | 1.44 | 1.45 | 18% | 1% | 20 (1×<) | 95% | 0% | 5% | |
| B | 12.9 | 12.4 | 14% | −3% | 21 | 95% | 5% | 0% | ||
| 4 | A | 5.82 | 5.85 | 20% | 0% | 17 | 100% | 0% | 0% | |
| B | 11.1 | 11.7 | 12% | 5% | 17 | 100% | 0% | 0% | ||
| 5cx-MEPP | 1 | A | 1 | 9.62 | 25% | - | 14 | 93% | 7% | 0% |
| B | 1 | 35.6 | 40% | - | 14 | 71% | 21% | 7% | ||
| 2 | A | 5.41 | 4.77 | 22% | −12% | 19 (1×<,1 FN) | 85% | 5% | 10% | |
| B | 33.0 | 29.7 | 21% | −10% | 20 | 85% | 5% | 10% | ||
| 3 | A | 3.22 | 2.55 | 36% | −21% | 19 | 89% | 0% | 11% | |
| B | 28.4 | 24.0 | 34% | −15% | 19 | 95% | 5% | 0% | ||
| 4 | A | 15.6 | 14.8 | 29% | −5% | 15 | 93% | 7% | 0% | |
| B | 24.7 | 23.3 | 30% | −6% | 15 | 93% | 7% | 0% | ||
| MnOP | 1 | A | 1 | 1.27 | 19% | - | 10 (1×<) | 80% | 0% | 20% |
| B | 1 | 6.13 | 17% | - | 11 | 82% | 0% | 18% | ||
| 2 | A | (0.179) 3 | 0.194 | 34% | 8% | 10 (4×<) | 64% | 14% | 21% | |
| B | 1.70 | 2.05 | 24% | 21% | 13 (1×<, 1 FN) | 79% | 14% | 7% | ||
| 3 | A | (0.402) 3 | 5 | 56% | - | 10 (4×<) | 80% | 0% | 20% | |
| B | 2.94 | 3.04 | 30% | 3% | 14 | 79% | 7% | 14% | ||
| 4 | A | 1.36 | 1.32 | 28% | −3% | 14 (2×<) | 92% | 8% | 0% | |
| B | 2.57 | 2.65 | 39% | 3% | 14 | 93% | 0% | 7% | ||
| OH-MiNP | 1 | A | (7.46) 1,6 | 5 | 82% | - | 8 | 7 | 7 | 7 |
| B | (17.5) 1,6 | 5 | 93% | - | 8 | 7 | 7 | 7 | ||
| 2 | A | 1.81 | 1.77 | 18% | −2% | 11 (2×<, 1 FN) | 85% | 8% | 8% | |
| B | 11.2 | 5 | 57% | - | 13 | 85% | 8% | 8% | ||
| 3 | A | 1.07 | 1.35 | 29% | 25% | 11 (3×<, 1 FN) | 67% | 25% | 8% | |
| B | (13.2) 3 | 13.9 | 26% | 5% | 14 | 79% | 7% | 14% | ||
| 4 | A | 5.80 | 5 | 51% | - | 11 | 82% | 0% | 18% | |
| B | 8.17 | 8.99 | 27% | 10% | 11 | 82% | 0% | 18% | ||
| cx-MiNP | 1 | A | (7.35) 1,6 | 5 | 69% | - | 10 (1×<) | 7 | 7 | 7 |
| B | 26.3) 1,6 | 5 | 70% | - | 10 (1×<) | 7 | 7 | 7 | ||
| 2 | A | 2.64 | 5 | 50% | - | 16 (1×<, 1 FN) | 53% | 24% | 24% | |
| B | 12.6 | 7.17 | 39% | −43% | 16 (1×<, 1 FN) | 63% | 19% | 19% | ||
| 3 | A | 2.04 | 2.11 | 47% | 3% | 17 | 82% | 12% | 6% | |
| B | 19.2 | 16.7 | 35% | −13% | 17 | 88% | 12% | 0% | ||
| 4 | A | 9.25 | 7.19 | 34% | −22% | 14 | 86% | 7% | 7% | |
| B | 15.7 | 12.8 | 30% | −19% | 14 | 86% | 0% | 14% | ||
| OH-MiDP | 1 | A | (6.90) 1,6 | 5 | 98% | - | 10 | 7 | 7 | 7 |
| B | (32.0) 1,6 | 5 | 101% | - | 10 | 7 | 7 | 7 | ||
| 2 | A | 2.88 | 5 | 85% | 13 (1×<, 1 FN) | 57% | 14% | 29% | ||
| B | 17.2 | 5 | 69% | 12 (2×<, 2 FN) | 71% | 7% | 21% | |||
| 3 | A | 1.55 | 1.65 | 29% | 6% | 15 | 100% | 0% | 0% | |
| B | 19.1 | 17.7 | 27% | −8% | 15 | 100% | 0% | 0% | ||
| 4 | A | 9.87 | 5 | 61% | 12 | 83% | 0% | 17% | ||
| B | 15.9 | 5 | 73% | 12 | 75% | 8% | 17% | |||
| cx-MiDP | 1 | A | (5.28) 1,6 | 8 | 2 (2×<) | 8 | 8 | 8 | ||
| B | (23.9) 1,6 | 8 | 2 (2×<) | 8 | 8 | 8 | ||||
| 2 | A | 1.95 | 8 | 10 | 80% | 0% | 20% | |||
| B | 10.0 | 8 | 10 | 90% | 0% | 10% | ||||
| 3 | A | 1.80 | 8 | 10 (1×<, 1 FN) | 91% | 0% | 11% | |||
| B | 14.6 | 8 | 11 | 100% | 0% | 0% | ||||
| 4 | A | 7.19 | 8 | 8 | 88% | 13% | 0% | |||
| B | 13.5 | 8 | 8 | 88% | 0% | 13% | ||||
| OH-MINCH | 1 | A | (3.28) 1,6 | 5 | 54% | 11 | 7 | 7 | 7 | |
| B | (19.1) 1,6 | 5 | 46% | 11 | 7 | 7 | 7 | |||
| 2 | A | 6.91 | 5 | 51% | 12 | 75% | 17% | 8% | ||
| B | 22.9 | 5 | 49% | 12 | 83% | 8% | 8% | |||
| 3 | A | 1.09 | 0.953 | 41% | −13% | 12 | 83% | 17% | 0% | |
| B | 13.0 | 10.7 | 19% | −18% | 12 | 100% | 0% | 0% | ||
| 4 | A | 12.3 | 9.69 | 32% | −21% | 11 | 91% | 0% | 9% | |
| B | 9.71 | 7.91 | 31% | −19% | 11 | 91% | 0% | 9% | ||
| cx-MINCH | 1 | A | (3.16) 1,6 | 5 | 70% | 10 | 7 | 7 | 7 | |
| B | (14.6) 1,6 | 5 | 57% | 10 | 7 | 7 | 7 | |||
| 2 | A | 3.67 | 5 | 55% | 11 | 82% | 9% | 9% | ||
| B | 12.1 | 5 | 70% | 11 | 82% | 9% | 9% | |||
| 3 | A | 1.09 | 5 | 53% | 10 | 80% | 10% | 10% | ||
| B | 8.30 | 5.04 | 15% | −39% | 10 | 100% | 0% | 0% | ||
| 4 | A | 7.07 | 8 | 9 | 89% | 11% | 0% | |||
| B | 7.70 | 8 | 9 | 89% | 0% | 11% |
| Performance | ||||
|---|---|---|---|---|
| N | Satisfactory | Questionable | Unsatisfactory | |
| R1 using corresponding analogue | 193 | 90% | 4% | 6% |
| R1 using other isotope label | 77 | 70% | 13% | 17% |
| R2 using corresponding analogue | 341 | 87% | 6% | 7% |
| R2 using other isotope label | 107 | 67% | 16% | 17% |
| R3 using corresponding analogue | 278 | 92% | 5% | 3% |
| R3 using other isotope label | 66 | 86% | 9% | 5% |
| R4 using corresponding analogue | 242 | 95% | 2% | 2% |
| R4 using other isotope label | 70 | 71% | 10% | 19% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mol, H.G.J.; Elbers, I.; Pälmke, C.; Bury, D.; Göen, T.; López, M.E.; Nübler, S.; Vaccher, V.; Antignac, J.-P.; Dvořáková, D.; et al. Proficiency and Interlaboratory Variability in the Determination of Phthalate and DINCH Biomarkers in Human Urine: Results from the HBM4EU Project. Toxics 2022, 10, 57. https://doi.org/10.3390/toxics10020057
Mol HGJ, Elbers I, Pälmke C, Bury D, Göen T, López ME, Nübler S, Vaccher V, Antignac J-P, Dvořáková D, et al. Proficiency and Interlaboratory Variability in the Determination of Phthalate and DINCH Biomarkers in Human Urine: Results from the HBM4EU Project. Toxics. 2022; 10(2):57. https://doi.org/10.3390/toxics10020057
Chicago/Turabian StyleMol, Hans G. J., Ingrid Elbers, Claudia Pälmke, Daniel Bury, Thomas Göen, Marta Esteban López, Stefanie Nübler, Vincent Vaccher, Jean-Philippe Antignac, Darina Dvořáková, and et al. 2022. "Proficiency and Interlaboratory Variability in the Determination of Phthalate and DINCH Biomarkers in Human Urine: Results from the HBM4EU Project" Toxics 10, no. 2: 57. https://doi.org/10.3390/toxics10020057
APA StyleMol, H. G. J., Elbers, I., Pälmke, C., Bury, D., Göen, T., López, M. E., Nübler, S., Vaccher, V., Antignac, J.-P., Dvořáková, D., Hajšlová, J., Sakhi, A. K., Thomsen, C., Vorkamp, K., Castaño, A., & Koch, H. M. (2022). Proficiency and Interlaboratory Variability in the Determination of Phthalate and DINCH Biomarkers in Human Urine: Results from the HBM4EU Project. Toxics, 10(2), 57. https://doi.org/10.3390/toxics10020057